Why India’s wastewater is a haven for superbugs that outdo medicines
Wastewater from homes, hospitals and pharma factories mixes together, creating the ideal breeding ground for drug-resistant bacteria







What happens once we press the flush valve in our bathrooms? In our heads, the waste swirls down into a deep, black void of no-place. We exit the bathroom, and all is forgotten. In reality, the journey that this wastewater embarks on is far less contained—often spilling out of underground pipes into open drains, leaking into the soil, or flowing directly into the rivers that run through our cities.
For many privileged urban Indians, this system remains invisible or beyond our sight, encountered only as the occasional overflowing drain during the monsoon, or the persistent stench along a riverbank. Yet India produces approximately 1,20,000 tonnes of faecal sludge daily, from just urban households. Add to this waste from hospitals, neighbourhood clinics, pharmaceutical manufacturing, and agricultural run-off and animal waste washing in from peri-urban farms—far more waste than we can comprehend. The end result is a potent cauldron in which bacteria from different sources can interact, alongside nutrients, antimicrobial drugs and their derivatives.
Pathogens in such wastewater can develop stronger resistance to the very medicines used to treat them, owing to the diverse microbial atmosphere they are swimming in, which encourages such evolution. Water has, in fact, played a significant role in the rise and spread of antimicrobial resistance (AMR). These potential superbugs, which have developed resistance to multiple antibiotics, can then re-enter our cities—and bodies—through contaminated sources and the water extracted from them.
Muddying the water
Surprisingly, agricultural run-off from peri-urban belts is the biggest culprit, contributing to nearly 80% of the antibiotic load entering urban sewage systems, says Dr. Rajesh Mishra, Director, Centre of Cellular and Molecular Biology, Hyderabad. “Animals and fields are primed with antibiotics to boost yields, which laces both groundwater and mixes with urban sewer pipelines. Improper disposal of antibiotics from households and hospital discharge also plays a role,” he adds. Troublingly, antibiotics are only partially absorbed by the body. Residual amounts (ranging between 30% - 90%!) are excreted through urine and feces—making the simple swing of a household flush valve neither innocent nor insignificant.
But it is difficult to single out the offender in this complex web. Untreated pharmaceutical effluents released into rivers also find their way directly into households as well as into sewage. Near Himachal Pradesh’s pharma hub Baddi, for instance, researchers found ciprofloxacin levels in the Sirsa river to be nearly 1,500 times higher than acceptable limits, likely due to industrial discharge. Another 2022 study by Toxics Link detected antibiotics such as ofloxacin, norfloxacin and sulfamethoxazole in rivers including the Yamuna, Gomti, Zuari and Cooum at concentrations two to five times above proposed safety limits.
Troublingly, antibiotics are only partially absorbed by the body.
Hospital sewage should ideally be treated before being released into sewer pipelines, says Dr. Atya Kapley, geneticist and Vice President of the Organisation for Women In Science for the Developing World. In reality, it contains faecal waste from large numbers of patients, many of whom are actively undergoing antibiotic treatment. This means that both antibiotic residues and bacteria from infected bodies enter the same sewage system together. A 2019 study examining effluents from a hospital in Mumbai found that the wastewater harboured an extraordinary diversity of antibiotic resistance genes and proteins—including carbapenemases, which confer resistance to last-resort antibiotics used for severe infections.
While this is a global concern, India has lacked detailed, location-specific data relevant to how AMR develops in wastewater. Two recent landmark studies attempt to address this gap. The first comprehensive map of resistant genes and microbes in the country’s largest metro cities of Mumbai, New Delhi, Chennai and Kolkata’s wastewater (conducted in 2026) demonstrates that although the dominant bacteria and microbial composition vary across cities, resistance mechanisms remain largely similar.
For example, the bacterium Klebsiella pneumoniae—associated with illnesses such as pneumonia and urinary tract infections—appeared more frequently in samples from Chennai and Mumbai. Klebsiella pneumoniae is one of the bacteria that produces highly versatile enzymes, which reduce the power of carbapenem antibiotics, used as a last line of defence.
Pseudomonas aeruginosa, which is linked to bloodstream and catheter-related infections, was more commonly detected in Kolkata. Yet across all the cities studied, researchers consistently found similar ‘resistomes’: the genes that help bacteria fortify their cell walls, neutralise antibiotics, or pump the drugs out of their cells.
The second study (conducted in 2025) analysed urban sewage microbiomes across six Indian states, collecting samples from hospital discharge as well. The study specifically examined samples from the Delhi-NCR region to study how compounds might appear downstream in the Yamuna river. They detected 11 widely used antibiotics spanning seven drug classes. Kanamycin appeared in 67% of samples and azithromycin in 56%. This speaks to how widespread the use and prescription of these antibiotics has become.
Also read: Typhoid lurks in India’s water. Why are antibiotics failing to stop it?
What the eye cannot see
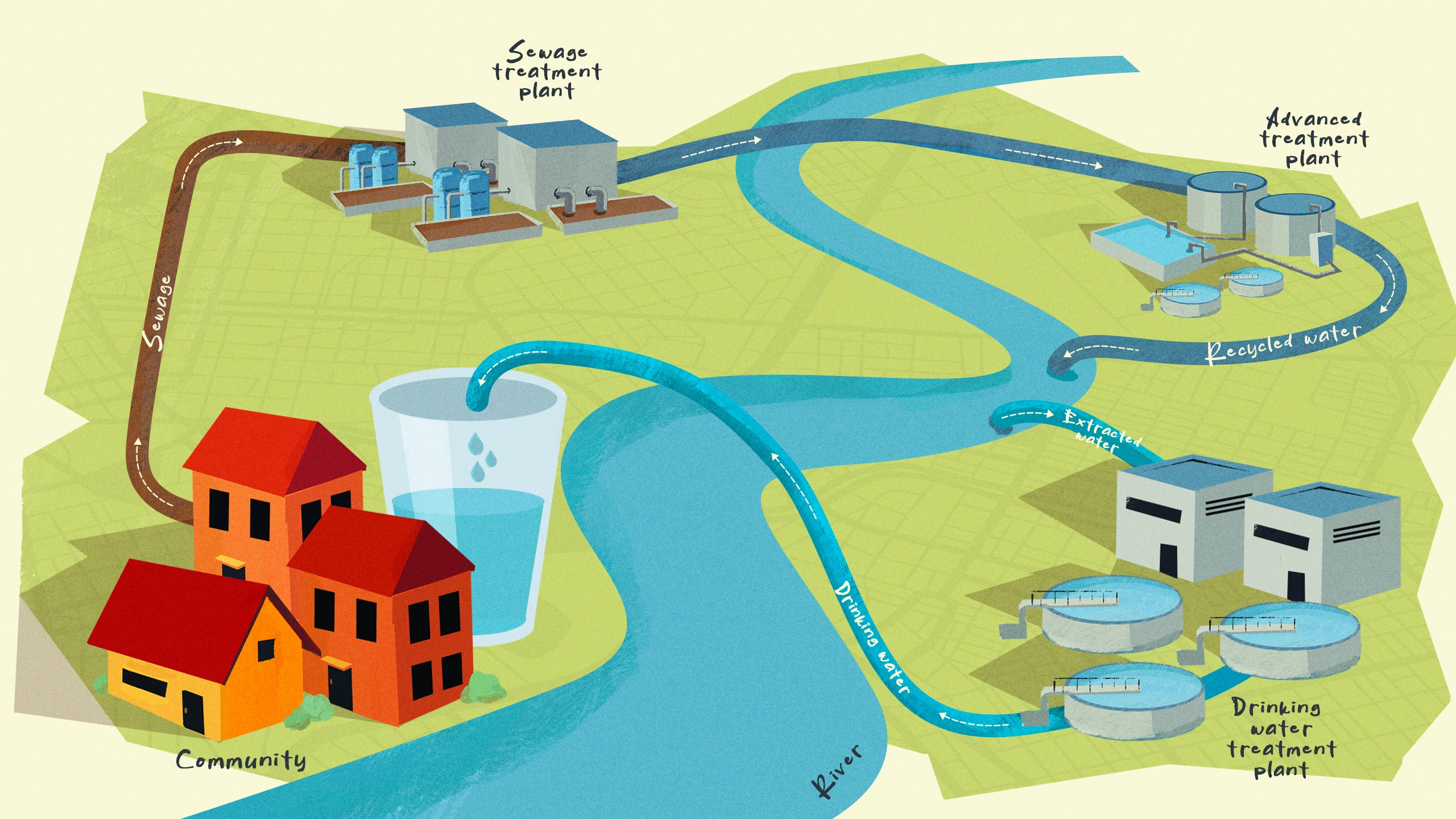
In an ideally planned and run city, wastewater follows a closed path, moving from homes and hospitals through underground sewers into treatment plants, where contaminants are removed before the water is released back into local water bodies and reused. But in much of urban India, this pathway is incomplete. By the time these different streams of wastewater converge, they have formed a nutrient-rich microbial concoction, ripe for bacteria to become stronger.
“Bacteria are extraordinarily diverse, with different cell walls and built-in defence systems that help them survive hostile conditions. When exposed to toxic substances like antibiotics, bacteria adapt: some develop mutations that make the drug ineffective, while others acquire resistance genes from neighbouring microbes, learning new ways to survive,” says Dr. Kapley.
Urban sewage systems then, are not just passive reservoirs where AMR accumulates, but where novel pathogens emerge.
In wastewater, antibiotics are frequently present in low, sub-lethal concentrations, which don’t kill microbes but push them to evolve resistance, says Dr. Karthik Tallapaka of the Centre for Cellular and Molecular Biology, the co-author of the 2026 watershed study mapping the persistence of AMR in urban sewage. "Add to this heavy metals and trace elements like mercury, boron and copper, which leach from pharmaceutical effluents and are also naturally present in soil, helping co-select for AMR,” he adds.
Very often, bacteria pack multiple useful genes together on the same mobile DNA element, which allow them to build and sustain resistance to multiple threats at once. For instance, one plasmid (a small circular DNA molecule that is home to genes with a survival edge) may carry resistance to a heavy metal like mercury, a chemical agent like a disinfectant and antibiotic resistance all in a single packet.
Polluted water kills weaker bacteria, and only bacteria carrying the stronger, whole packet, survive. And because the AMR gene is stored in the same packet, it survives too (even if antibiotics may not be present in that stream of wastewater at that time), continuing to persist in the environment as an AMR carrier. Similarly, disinfectants, fertiliser residue and personal care products also release chemicals like triclosan and parabens that exert selective pressure. These chemicals, present in low, sub-lethal concentrations in the water, kill some bacteria and encourage mutant, resistant strains to rise. For example, Chennai is a significant hub of industrial sulphur manufacture and use, present across its rubber and fertiliser sectors, which led to high concentrations of sulphur being found in the city’s wastewater.
The resistome is a vast universe where resistance is constantly being rapidly exchanged and conferred. This happens mainly through antibiotic-resistance genes (ARGs) of antibiotic-resistance bacteria and mobile-genetic elements (MGEs, or genes that are supple and can ‘jump’ from one place in a genome to another). Urban sewage systems then, are not just passive reservoirs where AMR accumulates, but where novel pathogens emerge.
The unfiltered truth
Can wastewater treatment plants (WWTPs) help reduce the intensity of AMR? WWTPs were originally built to remove visible and harmful pollutants like debris and large amounts of organic waste. Technology has advanced since then, but WWTPs still cannot fully remove ARBs. “Wastewater contains nanogram or picogram levels of antibiotics: difficult to measure in general tests, but enough to trigger AMR,” Dr. Kapley says.
Even when sewage treatment plants kill a bacterium, it cannot always erase its genetic traces.
This is alarmingly the best case scenario. Most sewage in India never finds its way to a treatment plant (of which many plants, in turn, fail to comply with discharge standards). Only about 40% of urban domestic waste is treated, says Dr. Kapley, and nearly 40 million litres of untreated sewage is released into rivers and other water bodies every day. The consequences are deadly.
“Even when sewage treatment plants kill a bacterium, it cannot always erase its genetic traces,” says Dr. Tallapaka. Fragments of their DNA, including antibiotic resistance genes persist, which can then occasionally be scavenged and feasted upon by other bacteria. How often this actually happens in wastewater, however, remains one of the big unanswered questions in AMR research. WWTPs, then, are another cog in this circular system that redistributes resistance instead of being a disposal endpoint.
Also read: How drug-resistant tuberculosis is bringing life to a halt in India
Living alongside AMR and wastewater
Partially treated wastewater also circulates through cities in ways we may never notice. In water-scarce regions, treated sewage water is routinely reused for construction, flushing toilets, cooling industrial systems, watering gardens and irrigating peri-urban farms that grow vegetables, rice and fodder crops for dairy cattle. A spinach field on the outskirts of a city may be irrigated with canal water containing sewage laced with pharmacological compounds; a dairy animal may drink from a contaminated pond; fish may breed in rivers receiving untreated effluents. During monsoons, overflowing drains and flooded sewer lines can mix with groundwater and lakes from which water is later drawn for domestic treatment and supply. Even activated sludge—the dense, microbe-rich residue separated during wastewater treatment—is sometimes repurposed as fertiliser or dumped in open landfills, where resistant bacteria and ARGs may persist in soil and run-off, says Dr. Mishra.
The urban citizen (us!) encounters these pathways in everyday life. The exposure may come through, say, coriander washed in contaminated water and sprinkled raw onto street food, milk from cattle exposed to polluted fodder and water, or produce grown along riverbanks downstream of sewage discharge. A child playing in floodwater after heavy rain, or a resident living beside an open drain inhaling aerosolised wastewater particles, may encounter microbes shaped by these environments. Infants are especially prone to a compromise of long-term health. “Adults have years of immune experience behind them. Infants do not. So when a resistant bacterium enters a newborn’s body, it can meet an immune system that is still under construction, while treatment options become constricted,” adds Dr. Mishra.
Wastewater surveillance may become one of the most important tools in tracking the spread of antimicrobial resistance.
With manual scavenging of waste being a reality in India’s caste-segregated ecosystem, people on the margins—like Dalit communities—are on the frontlines of the AMR crisis, and that much more likely to be afflicted with disease. The burden of battling longer and more persistent infections also falls on a demographic that has little to no resources, engaged in labour that strikes at their dignity and who have few rights in India’s health economy.
Wastewater surveillance may become one of the most important tools in tracking the spread of antimicrobial resistance. “The first thing we need is baseline data,” says Dr. Tallapaka. “Using newer genome-sequencing technologies, we are now able to study sewage as a kind of biological snapshot of a city,” he adds. But much of what scientists are detecting appears to be novel. Establishing long-term surveillance systems could help researchers identify emerging resistance patterns and perhaps even provide early warning signs of future outbreaks. “Ideally,” says Dr. Tallapaka, “wastewater should provide a bird’s-eye view of whatever is happening in the [microbial] community.”
There are a host of reasons to better treat wastewater and sewage, from the preservation of aquatic ecosystems, to the bolstering of the health of communities who depend on a source of water, and its sustainable reuse in a warming world. The persistence of AMR is only one amongst many things at stake.
Also read: Add crisis to cart: Why instant delivery and antibiotics don't mix
Cover Art by Khyati K
{{quiz}}


.avif)
Explore other topics
References